
by Karen Sheffler, MS, CCC-SLP, BCS-S
Inspiration for this blog from:
“When the cause of dysphagia is not obvious:
Sorting through treasure and surprises in the medical record”
by James L. Coyle, PhD, CCC-SLP, BCS-S
April 11, 2014 at the ASHA Healthcare & Business Institute
Medicine has its uncertainties. This may cause the speech-language pathologist to be very conservative, possibly over-treating or overcompensating, per James Coyle, PhD, CCC-SLP, BCS-S at his talk on April 11, 2014.
Coyle advised clinicians to value the medical record just as much as our direct examination of the patient.
The “medical record is a messy place,” per Coyle, so dig in there and get messy.

Digging through the medical record can be messy!
This job becomes easier as hospitals are switching to electronic medical records. A patient’s inpatient and outpatient history, as well as the current condition, should be a few clicks away.
It is our job to dig for clues to distinguish which came first: the illness or the dysphagia. Some conditions can mimic dysphagia-related aspiration pneumonia. Some community acquired infections can create weakness and delirium, which then cause an acute dysphagia.
I have summarized Dr Coyle’s talk into these seven clues or questions:
-
Is it pneumonia?
-
What type of pneumonia is it?
-
What was the patient’s baseline?
-
Is there a systemic spread of infection, or septicemia (aka: sepsis)?
-
Was there a surgical procedure that could have caused the dysphagia?
-
Was there a medical procedure that could have caused the dysphagia or an aspiration?
-
Are there medications that could be causing the dysphagia?
Let’s start with a common story:
An active and independent elderly female develops a urinary tract infection (UTI). She feels sleepy and stops eating and drinking regularly. This worsens the UTI and causes dehydration. She gets to the hospital 4 days after the onset of symptoms. Dehydration causes electrolyte imbalances, leading to delirium. Delirium plus infection equal more lethargy and a global cognitive decline. Being out of her usual environment causes more confusion and agitation. Antipsychotic medications are used to control the acute agitation. The patient becomes septic, as the infectious process spreads. Her urosepsis spreads to a pneumonia. She stops eating and drinking. The nurse reports that she choked on her medications, leading the doctor to order a bedside swallowing evaluation. The speech-language pathologist (SLP) notes a high aspiration risk, as the patient looks severely impaired. Unfortunately, there was no time that day for the thorough chart review that is the clinician’s standard practice. The patient is labeled with severe dysphagia and a dysphagia-related aspiration pneumonia. She stays on thickened liquids and pureed foods. It could be worse, the patient may have been labeled so severely dysphagic that she was given a feeding tube and ordered not to not eat or drink anything. Will the patient fall through the cracks and never eat regular food again, or will an SLP re-evaluate her in two weeks and discover that her dysphagia has disappeared? To be continued…
7 CLUES IN THE MEDICAL RECORD TO DISCOVER DYSPHAGIA:
-
IS IT PNEUMONIA?
What is pneumonia? Coyle described the infectious process as: inhaled or aspirated microorganisms/pathogens (which could be bacterial or viral). The pathogen colonizes the lung and draws nutrients out of the host. This destructive invasion damages tissue and causes inflammation. The pathogens reproduce and make waste, which further irritate and cause inflammation. Coyle recommended Ware & Matthay (2000) for a tutorial on the tissue trauma that occurs with severe inflammation.
The challenging differential diagnosis of pneumonia:
-
-
-
-
New infiltrate on CXR

Typically in the dependent bases of the lung if aspiration, but not necessarily only the right lower lobe if the patient is bedridden or aspirating while laying down on the couch.
-
Leukocytosis (WBC count of >11.5-12.0).
Warning: if the patient is immune compromised, they cannot make white blood cells. They are not capable of developing a leukocytosis. Check if the Neutrophil count is low.
-
Fever (>38 Celsius for >24 hours).
This would be a temperature increase of >1 degree over the normal of 37. That is important to know as we do not think in Celsius here in America!
-
Symptoms: change in mental status, increased respiratory rate, cough, and may have respiratory distress.
Note: as you watch the patient while he/she is eating and drinking, do not mistake that baseline cough for a cough from the sip of water you just gave him. Observe the cough for a while before beginning eating and drinking trials.
-
Sputum production: Analysis of a sputum sample is not always performed. It could be contaminated with the nasty pathogens from the patient’s mouth, unless taken directly from a bronchoalveolar lavage.
-
-
-
-
-
WHAT TYPE OF PNEUMONIA IS IT? This requires some hunting in the medical record. Doctors count on the evaluation by a speech-language pathologist to determine if the condition could be related to dysphagia and aspiration.
-
-
-
-
-
Ventilator Acquired Pneumonia (VAP): widespread infiltrates as the ventilator blows the pathogens into the lungs. There is typically a strong correlation with oral pathogens.
-
Dysphagia-Related Aspiration Pneumonia (DAP): was an oropharyngeal dysphagia present prior to the time of infection? Aspiration pneumonia typically shows up on CXR as tracking down the secondary bronchus into the lower lobe on the right-hand side, per Coyle. In addition to “infiltrates” on the radiologist’s report, you may see “ground-glass opacities,” which may be from chronic aspiration of particulate matter. A newer term, per Coyle, is “Diffuse Aspiration Bronchiolitis,” which also refers to chronic recurrent aspiration of particulate matter, showing up as specks of scarring.
What may seem to be a recurrent pneumonia may really be one big infection from ongoing dysphagia and aspiration. The patient needs a swallow study to determine if dysphagia is present and why. This is so important, because if we label them with DAP, that patient will forever have the words “Aspiration Pneumonia” in their past medical history. Then medical personnel may be overly conservative in the future.
Also consider causes and issues of dysphagia-related aspiration pneumonia:
-
-
-
-
-
-
-
-
-
-
Esophageal dysphagia with back-flow of contents to airway
-
Oral pathogens aspirated with secretions, food, and liquids.
-
Immune-compromised and bedridden patients who are dependent for oral cares and dependent feeders are at a much higher risk.
-
What was the volume and frequency of the aspiration?
-
What was the pH of the material aspirated?
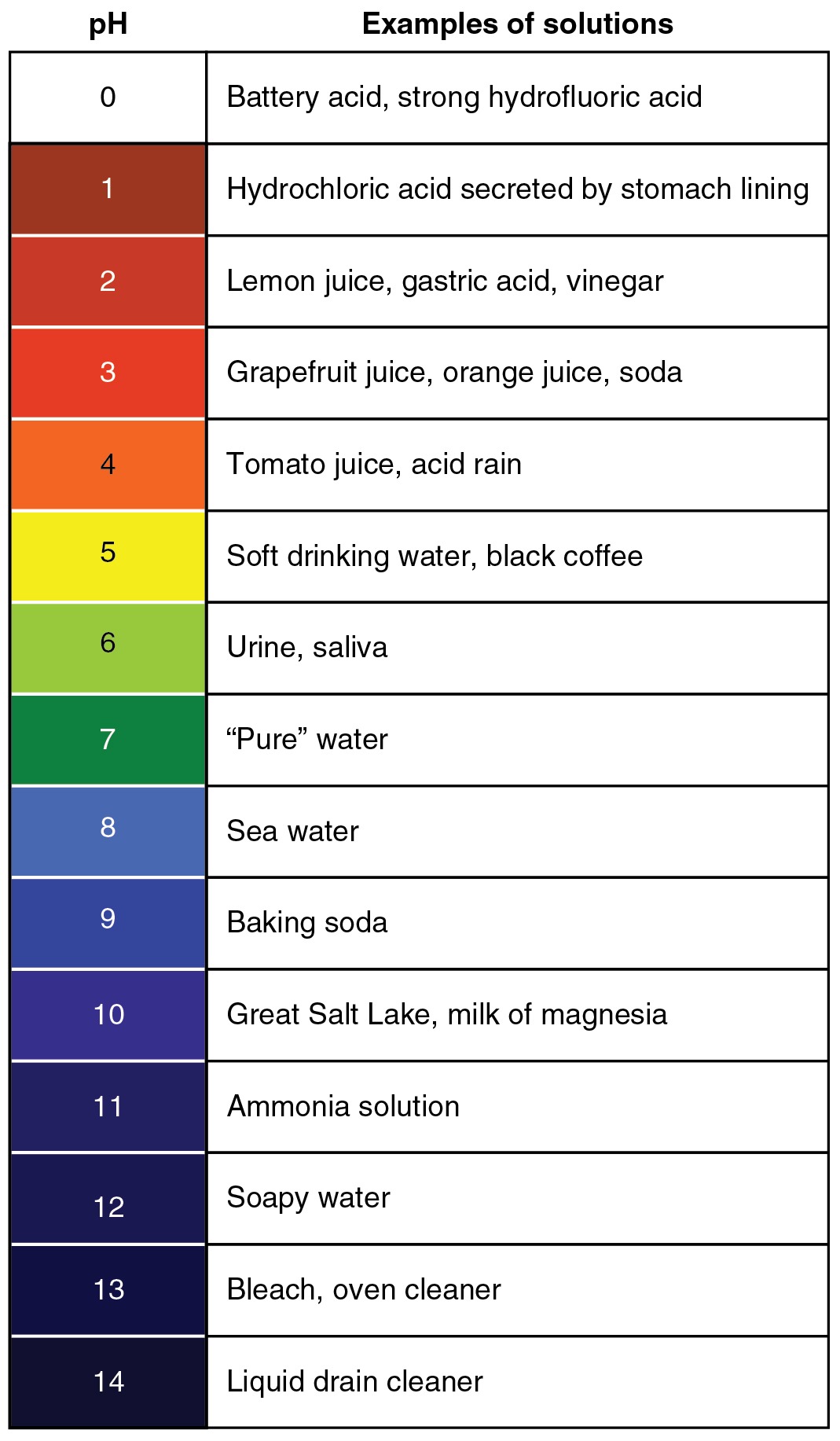
pH Scale. Note how pH of saliva should be a fairly neutral 6.
-
-
-
-
-
-
Non-Dysphagia-Related Aspiration Pneumonia (NDAP) and/or Aspiration Pneumonitis: if no oropharyngeal dysphagia present before infection, check history for chemical irritants, allergens, radiation therapy, reflux, a vomiting event, or use of acid-suppression therapy (H2Blockers or Proton-Pump Inhibitors).
-
-
-
-
Is there truly an infectious component?
-
A medicated stomach (via H2 Blockers or Proton-Pump Inhibitors for reflux) has the acid suppressed, and all sorts of bugs can grow in an alkaline environment.
-
Is it Aspiration Pneumonitis that does not require the pre-emptive use of antibiotics?
-
An unmedicated stomach has sterile-acidic gastric contents that burn and cause an acute lung injury. There is inflammation of the airway and alveoli due to the irritant.
-
Coyle recommended Marik (2001).
-
-
-
-
-
-
-
-
-
-
Hospital Acquired Pneumonia (HAP) or Healthcare-Associated Pneumonia (HCAP): highly likely related to an aspiration (see numbers 1-3 above). Nasty pathogens from the institution getting into the lung.
-
Community Acquired Pneumonia (CAP): tends to have a more diffuse distribution of infiltrates or not in the dependent lobes as in aspiration pneumonia. Need to know how the patient was prior to infection. Was dysphagia and aspiration present prior to infection?
-
-
-
-
-
WHAT WAS THE PATIENT’S BASELINE?
“You got to have dysphagia to have dysphagia,” joked Coyle. “But seriously,” he added, “I can’t underscore this enough.” To figure out if the pneumonia was a Dysphagia-Related Aspiration Pneumonia (DAP), the patient had to have had some difficulty swallowing prior to getting sick.
Be a detective. Look carefully in the medical record and at the past medical history.

-
-
-
-
Any conditions or diseases that could cause dysphagia?
-
Baseline nutritional status? A reduction in muscle mass (sarcopenia) from prolonged Protein Energy Malnutrition (PEM) could be a factor in causing the swallowing problem.
-
Call the nursing facility, talk to the patient, and ask the family (with permission, of course).
-
Tutorials: Schindler (2002) and Ney, et al (2009) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2832792/pdf/nihms178630.pdf
-
-
-
-
IS THERE A SYSTEMIC SPREAD OF INFECTION OR SEPTICEMIA (aka: SEPSIS)?
What is sepsis? Colye described how the infection can progress to the point that it breaks through the organ’s tissue barrier into the blood. For example, an aspiration pneumonia untreated could penetrate the alveoli into the pulmonary capillaries and spread through the circulatory system. There is a leakage of plasma volume, which causes low blood pressure (hypotension). Organs that depend on high blood pressure are damaged. When this commonly affects the kidneys, it is called an acute kidney injury. There can also be an acute brain injury due to sepsis. Sepsis can lead to multi-organ failure and death. Coyle noted that sepsis has a 60% mortality rate in the elderly. The medical team works to disrupt this sequence.
-
-
-
-
SOURCE: Our dependent elderly patients are especially vulnerable. The lung is not the sole source of the primary infection.
A dependent elder with poor hygiene may have E-coli gram-negative rods inoculating the bladder. A bad urosepsis (septic urinary tract infection) can even spread to a hematogenous pneumonia. This may be a patient who never had dysphagia prior, but is at risk for developing acute dysphagia due to the severity of the illness. The primary infection may also be in the oral cavity or a festering wound.
-
-
-
-
-
-
-
PROBLEM: The patient may not develop sudden signs. They may be just sleepy for a few days, but then it can unfold rapidly.
-
-
-
WARNING: Coyle urges speech-language pathologists to be careful when predicting goals for the future, as “sick people look pretty darn sick.” We evaluate function and ensure the patient’s safety while they are sick. Then good communication is needed at discharge to ensure re-evaluations. I have seen this pattern in patients with Multiple Sclerosis who develop urosepsis, as it would lead to a severe acute dysphagia. Then on their repeat Modified Barium SwallowStudy.com or FEES 2-3 weeks later, they would demonstrate baseline functioning and return to a regular diet.
-
ASK THE MEDICAL TEAM QUESTIONS: Is this a short-term reversible problem? Is this an acute delirium or a progressive decline due to a baseline of a chronic dementia? What is the natural progression of this illness or disease? When the delirium or sepsis goes away, will the patient return to his baseline OR do we expect permanent damage and a new baseline?
-
-
-
-
WAS THERE A SURGICAL PROCEDURE THAT COULD HAVE CAUSED THE DYSPHAGIA?
For examples: cardiothoracic surgery, procedures involving the chest wall, lung transplant, lung resection, esophagectomy, head and neck cancer resection, thyroid surgery, and more.
Was the phrenic nerve or the vagus nerve injured? The wandering vagus nerve with its left recurrent laryngeal nerve branch wraps around the aorta before it innervates the left true vocal cord. See post on cranial nerves.
-
-
-
-
Coyle recommended Atkins, et al (2007) re esophagectomy and lung transplantation.
-
Helpful review of peripheral nerve injuries during cardiac surgeries: Sharma, et al (2000).
-
Risk factors for vocal cord paralysis after cardiovascular surgery: Itagaki, et al (2007) found incidence of 2.3% new paralysis in 987 patients who survived cardiovascular surgery. Highest risk: Aortic procedures (especially descending aortic surgery) versus coronary artery bypass grafting, prolonged operation time, patients with hypertension, and all cases when the intubation time was greater than 100 hours.
-
-
-
-
WAS THERE A MEDICAL PROCEDURE THAT COULD HAVE CAUSED THE DYSPHAGIA OR AN ASPIRATION?
For examples: feeding tubes, prolonged intubation, traumatic intubation, repetitive extubations and re-intubations, self-extubations, peri-operative aspiration event, radiation to the head/neck/chest, and more.
-
-
-
-
Intubation: Baker, et al (2009) studied 254 patients who required intubation longer than 48 hours after cardiac surgery. 51% of these patients had post-extubation dysphagia, typically with pharyngeal stage impairment. The average number of hours from extubation to oral intake was 76.6 hours. The presence of dysphagia was the most important factor causing delays in oral intake and discharge.
-
The presence of a feeding tube has been shown to increase pneumonia rates:
-
-
-
-
-
-
-
-
-
Coyle recommended Segal, et al (2006), Wagner, et al (1994), and Dzeiwas, et al (2004) and (2008).
-
Segal, et al (2006) found a correlation between high gastric pH (alkaline stomach due to tube feeding) and the presence of pathogenic bacteria. Additionally, the same bacterial organisms colonizing the stomach were present in the mouth (frequently gram-negative bacteria and E coli). The presence of pathogenic oral bacteria was greater in patients with an NG tube (54%) versus a PEG (44%). This suggests that NG tube fed patients have more reflux to the oral cavity?
-
Dzeiwas, et al (2008) found that 44% of stroke patients with NG tubes in place developed pneumonia, even in the absence of a worsening dysphagia.
-
Langmore (1998 and 2002) found that tube feeding is one of the best predictors in whether a patient gets sick with aspiration pneumonia. Langmore stated: “Tube feeding promotes colonization because oral hygiene is often neglected in these patients and their salivary flow is often reduced.”
-
Feinberg, et al (1996) followed 152 nursing home patients for three years. They found that pneumonia wasmore common in the patient group with “major aspiration history AND artificial feeding” versus the “major aspiration with oral feeding.”
-
-
-
-
-
-
ARE THERE MEDICATIONS THAT COULD BE CAUSING THE DYSPHAGIA?
-
-
-
-
Polypharmacy: Langmore, et al (1998), found patients on multiple medications had a 15% increased risk of pneumonia.
-
Sedating medications. For examples: Lorazepam (Ativan), Gabapentin (Neurotin).
-
Antipsychotics (i.e., Haldol): Coyle recommended reading Knol, et al (2008). This was a case controlled study of elderly patients with age-matched controls. Patients who received antipsychotics where 60% more likely to have pneumonia.
-
Xerostomia (dry mouth). For examples: anticholinergics, antihistamines, antidepressants, antipsychotics, antiemetics (i.e., Scopolamine), antiparkinsonian, antihypertensives, opiates.
-
Esophagitis. For examples: antibiotics, steroids, non-steroidal anti-inflammatories (NSAIDS) like Ibuprofen, Warfarin, Diazepam, Phenobarbital.
-
Gastroesophageal reflux: Medications that lower the tone of the lower esophageal sphincter have increased risk for reflux aspiration. For examples: calcium-channel blockers (Diltiazem), alcohol, and even chocolate!
-
-
-
Hope you have enjoyed digging up these 7 treasures buried in the medical record.
Our answers to these questions have a great impact on all we do: from our initial direct examination to our discharge plan, and all the steps in between (e.g., patient/family education, communication with the team, recommendations, referrals, and the treatment plan).
Future blogs will cover oral hygiene and medications more in depth.
Important References from Coyle’s talk:
- Atkins, B. Z., Fortes, D. L., & Watkins, K. T. (2007). Analysis of respiratory complications after minimally invasive esophagectomy: preliminary observation of persistent aspiration risk. Dysphagia, 22(1), 49-54.
- Atkins, B. Z., Trachtenberg, M. S., Prince-Petersen, R., Vess, G., Bush, E. L., Balsara, K. R., . . . Davis Jr, R. D. (2007). Assessing oropharyngeal dysphagia after lung transplantation: altered swallowing mechanisms and Increased morbidity. The Journal of Heart and Lung Transplantation, 26(11), 1144-1148.
- Dziewas, R., Ritter, M., Schilling, M., Konrad, C., Oelenberg, S., Nabavi, D. G., . . . Ludemann, P. (2004). Pneumonia in acute stroke patients fed by nasogastric tube. Journal of Neurology, Neurosurgery & Psychiatry, 75(6), 852-856.
- Dziewas, R., Warnecke, T., Hamacher, C., Oelenberg, S., Teismann, I., Kraemer, C., . . . Schaebitz, W. R. (2008). Do nasogastric tubes worsen dysphagia in patients with acute stroke? BMC Neurology, 8, 28.
- Knol, W., van Marum, R. J., Jansen, P. A., Souverein, P. C., Schobben, A. F., & Egberts, A. C. (2008). Antipsychotic drug use and risk of pneumonia in elderly people. Journal of the American Geriatrics Society, 56(4), 661-666.
- Langmore, S. E., Terpenning, M. S., Schork, A., Chen, Y., Murray, J. T., Lopatin, D., & Loesche, W. J. (1998). Predictors of aspiration pneumonia: how important is dysphagia? Dysphagia, 13(2), 69-81.
- Marik, P. E. (2001). Aspiration pneumonitis and aspiration pneumonia. New England Journal of Medicine, 344(9), 665-671.
- Marik, P. E., & Kaplan, D. (2003). Aspiration pneumonia and dysphagia in the elderly. Chest, 124(1), 328- 336.
- Marik, P. E., & Zaloga, G. P. (2003). Gastric versus post-pyloric feeding: a systematic review. Critical Care (London). 7(3), R46-R51.
- Segal, R., Dan, M., Pogoreliuk, I., & Leibovitz, A. (2006). Pathogenic colonization of the stomach in enterally fed elderly patients: Comparing percutaneous endoscopic gastrostomy with nasogastric tube. Journal of the American Geriatrics Society, 54(12), 1905-1908.
- Wagner, D. R., Elmore, M. F., & Knoll, D. M. (1994). Bacterial contamination of enteral feeding reservoirs. Journal of Parenteral & Enteral Nutrition, 18(6), 562-Dec.
- Ware, L. B., & Matthay, M. A. (2000). The acute respiratory distress syndrome. The New England Journal of Medicine, 342(18), 1334-1349.
Other references:
- Barker, J., Martino, R., Reichardt, B., Hickey, E. J., & Ralph-Edwards, A. (2009). Incidence and impact of dysphagia in patients receiving prolonged endotracheal intubation after cardiac surgery. Canadian Journal of Surgery, 52 (2), 119-124.
- Feinberg, M. J., Knebi, J., & Tully, J. (1996). Prandial aspiration and pneumonia in an elderly population followed over 3 years. Dysphagia, 11 (2), 104-109.
- Itagaki, T., Kikura, M., & Sato, S. (2007). Incidence and risk factors of postoperative vocal cord paralysis in 987 patients after cardiovascular surgery. Ann Thorac Surg, 83, 2147-2152.
- Langmore, S. E., Skarupski, K. A., Park, P. S., & Fries, B. E. (2002). Predictors of aspiration pneumonia in nursing home residents. Dysphagia, 17 (4), 298-307.
- Ney, D., Weiss, J., Kind, A., & Robbins, J. (2009). Senescent Swallowing: Impact, strategies, and interventions. Nutr Clin Pract., 24 (3), 395-413. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2832792/pdf/nihms178630.pdf
- Schindler, J.S. & Kelly, J. H. (2002). Swallowing Disorders in the Elderly. The Laryngoscope, 112, 589-602.
- Sharma, A. D., Parmley, C. L., Sreeram, G., & Grocott, H. P. (2000). Peripheral nerve injuries during cardiac surgery: Risk factors, diagnosis, prognosis, and prevention. Anesth Analg, 91, 1358-1369.
This is truly informative, loved reading it.! Gained so much out it n got a new perspective.! Looking forward for the more information.!
Thanks. Hope you enjoy the new posts on Oral Hygiene and Aspiration Pneumonia.