
Truth is Stranger than Fiction – What is in Your Dysphagia Toolbox?
(Part 3)
By guest blogger: Amanda Warren, MS, CCC-SLP
Edited by Karen Sheffler, MS, CCC-SLP, BCS-S of SwallowStudy.com
Thanks for reading Part 1 and Part 2 of our of our Truth Is Stranger Than Fiction series. You’ve found the last installment, part 3 in this 3 part series summarizing 5 more sessions at the 2018 Dysphagia Research Society’s (DRS) Annual Meeting. And remember, these are not the only topics that were covered at this year’s DRS, nor are they even the most important. But they were a few that made me think the most. So read on. You might just learn that even in the field of dysphagia, truth is stranger than fiction.
11. The Effortful Swallow is more effective with larger, more viscous boluses.
From session titled Effect of effortful swallow on pharyngeal cavity volume with 10 ml honey-thick boluses: Kinematic analysis using 3D dynamic Computed Tomography presented by Dr. Yoko Inamoto
Dr. Yoko Inamoto from Fujita Health University gave a beautiful talk about the use of 3-D CT to measure the oropharyngeal swallow in 7 heathy participants who were free from any dysphagia. She compared their function while performing a typical swallow and again while performing an effortful swallow. Results revealed a significant difference with effortful swallows in the duration of swallow and offset of pharyngeal squeeze.
In other words, the pharyngeal cavity volume was smaller for a longer time when the individuals were performing an effortful swallow than when they were performing a typical swallow. Of most interest to me was that the findings were more significant with larger, more viscous boluses than with smaller, thinner boluses.
So, it made me wonder, how often do we shy away from larger bites and larger sips due to worries about aspiration or residue build-up? I know I have heard: “we’re only doing ice chips right now” or “small sips only” in clinical recommendations. When paired with a swallow strategy and exercise such as the effortful swallow, should we liberalize these consistencies or volumes in order to maximize their effects? This needs to be in our dysphagia toolbox to at least attempt larger bites and sips of varying viscosities under the supervision of an instrumental examination (you have that suction unit ready). Of course, plenty more work needs to be done. We cannot clearly extrapolate a small study on only normal healthy participants with 100% confidence, but it was definitely food for thought during my time at DRS this year.
12. Attention to task impacts laryngeal and pharyngeal awareness and the urge to cough.
From session titled Attentional resource allocation and cough reflex sensitivity in healthy young individuals presented by Dr. Sarah Perry
Dr. Sarah Perry, along with her colleagues in The Laboratory for the study of Upper Airway Dysfunction (UAD), led by Dr. Michelle Troche, made waves with their recent study on how attention to task impacts cough function. In her work, Dr. Perry evaluated the cough reflex of 28 healthy participants both with and without the distraction of a tone discrimination task. She measured the lowest amount of stimuli that would elicit a cough, the severity of urge to cough, and the overall strength of the cough when it did occur. She found some fascinating results! Her subjects, when distracted:
- coughed less frequently,
- had reduced urge to cough, and
- required more stimuli to produce a cough.
Wow, right? She did find that the strength of the cough, once it occurred, was equal in the two scenarios.
I honestly cannot stop thinking about this study and cannot wait to see where she goes with it next. Here’s why. Think for a second… do you factor distractions into your management plan? Sure, we all do, right? We recommend “reduce distractions during meals” in our list of safe swallowing strategies and aspiration precautions. But do you explain why to your patients (and their families or the nursing staff)? Do you follow up to ensure your recommendations are actually happening? Also, what about distractions present when providing group treatment? In a time period where productivity is king and group therapy is encouraged, should you really be administering therapy to groups for your patients with dysphagia? Are we factoring in the added distractions in our goals? Are you assuming your patient is getting better due to “less coughing,” when in reality his urge to cough was reduced due to the distracting setting.
Let’s consider this distraction issue further: You may factor distractions into your dysphagia toolbox for therapy, but do you factor it into your instrumental evaluations regarding patient response to aspiration? What can your patient see and hear during their Videofluoroscopic SwallowStudy.com (VFSS, aka MBSS) or Fiberoptic Endoscopic Evaluation of Swallowing (FEES)? I can think of more than a few patients who are totally visually distracted by seeing the screen during a VFSS. Sure, visual feedback can be a very useful therapy tool (see Alicia Vose’s work in #7 of part 2 of this series for starters!), but… what if a visual or auditory distractor during your evaluation has impacted someone’s urge to cough or frequency of cough? Could you, in theory, be labeling them at higher risk due to observing silent aspiration on your study? How would that change your plans for reassessment? We need so much more work in this area of the intersection of attention/cognition/responsiveness and swallowing function (aka, psychophysics). I look forward to reading more of Dr. Perry’s work in the future!
On an editor’s side-note: When no cough response to aspiration is seen on an instrumental exam, we assume that the reason is a lack of sensation at the level of the larynx, vocal cords and within the top of the trachea. There may be an issue with the complex thermoreceptors, chemoreceptors and mechanoreceptors above and below the vocal cords, and we may start blaming the superior laryngeal nerve and recurrent laryngeal nerve branches of the Vagus. Now Perry and Troche’s research suggests that it may be further complicated by distractions as well. Additionally, there is little research on sensation itself! (Consider checking out the second episode in the 2017 DysphagiaGrandRounds.com by Dr Ianessa Humbert and Rinki Varindani Desai to hear a robust discussion of some sensory research studies. They specifically reviewed an article called: “Oral Perception of Liquid Volume Changes With Age;” https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4578969/. This research noted that older individuals already have a higher threshold for orally perceiving bolus volume changes, and now this current DRS study showed that distractions can affect people’s sensory thresholds too).
This complexity is further highlighted in a study published in May 2018 by Dr Anna Miles and team (see title and link at the bottom of this paragraph). They found significant variability in patients’ responsiveness across different viscosities and volumes. Surprisingly, some patients responded with a cough when they aspirated thin liquid, but did not cough when they aspirated a mildly thick liquid (per www.IDDSI.org framework; aka, nectar thick liquid). This sensory response discrepancy is very concerning, as how many times at the bedside do we see a cough on thin liquid, and then we do not see any distress on a thickened liquid? We assume that the thicker liquid was “tolerated” better, right? Miles and her colleagues warned that therapists should not classify patients as “silent aspirators” versus “overt aspirators,” as there can be such variability within a patient, based on volume and viscosity (and on distractions as we learned from above!) This study gives you all the more reason to advocate for instrumental evaluations. See “Cough response to aspiration in thin and thick fluids during FEES in hospitalized inpatients,” by Anna Miles, Mary McFarlane, Samantha Scott, and Alexandra Hunting; https://onlinelibrary.wiley.com/doi/abs/10.1111/1460-6984.12401
13. Lymphedema therapy has significant impacts on swallow function and perception in patients with dysphagia secondary to head and neck cancer.
From session entitled Understanding the impact of head and neck lymphedema on swallow function: Insights from patients’ experiences presented by Claire Jeans
The title for this one alone may be super obvious to some of you, if you happen to specialize in head and neck cancer evaluation and treatment. For others, like me, maybe this population is only a small portion of your caseload. Have you distinguished the ways in which this patient population is drastically different than the others that you are evaluating and treating? I encourage you to read up on the topic more! There’s amazing work being done about best practices for patients who are pre-treatment, mid-treatment for their cancer and at various stages of the post-treatment life. Head and neck cancer competency is important for diagnosing, treating, and making appropriate referrals!
The need to make appropriate referrals is how this study stood out for me. Claire Jeans from Calvary Mater Hospital Newcastle in Australia presented great background information first, showing us previous research on how the Penetration Aspiration Scale (PAS) scores and Functional Oral Intake Scale (FOIS) scores are worse for patients when lymphedema is present (see work by Deng, et al., 2012, Jackson, et al., 2016, and Deng, et al., 2013 if you want to dig into that more). She next identified that in all that literature, there was no research on patient perception and sensation when lymphedema is present. Ms. Jeans and colleagues studied 12 participants who were over 3 months post chemotherapy and radiation treatment for their head and neck cancer. They gathered information about their sensation and perception of discomfort throughout the day. Results indicated that the majority of participants (11/12, 92%) reported tightness and changes which impacted both their comfort and their diet tolerance.
Just hearing her data really made me think, as a provider who is not trained or qualified to provide lymphedema treatment myself, do I ask enough questions of my patients who might be struggling with lymphedema? Even if I am not qualified to provide the treatment myself, the more I know and study the benefits, the better advice I will be able to provide my patients in the future. Do I refer out to my trained colleagues as frequently as I should? If I did refer more, would we as a team be providing better overall holistic patient care with an improved quality of life for this sub-group of my overall caseload?
14. Resistance training is possible for the laryngopharynx, if you have the right tools in your dysphagia toolbox.
From session titled Rehabilitation of a Heterogeneous Group of Dysphagic Patients by a Novel Exercise Technique of Swallowing Against Laryngeal Restriction presented by Dilpesh Agrawal
If you are an SLP who is stuck in the mindset that device-assisted swallowing therapy is new-fangled or not-yet-proven, I urge you to get yourself to Dysphagia Research Society’s annual conference next year if for no other reason than to listen to all of the amazing work being done with devices you have never heard of. I’d encourage you to listen and think to yourself: “what tools are in my dysphagia toolbox?” or “Do I have access to everything I need to actually help my patients improve?” Challenge yourself and your team to advocate to get access to tools which are research driven and actually proven to make a change in patients’ lives.
At DRS, I was introduced (maybe late to the game?) to an exercise regimen called Swallowing Against Laryngeal Restriction (SALR) by Dr. Dilpesh Agrawal and his colleagues at Medical College of Wisconsin (where Dr Reza Shaker, MD is the Chief Director). By strapping this device externally to the front of the neck where it can provide restriction or resistance to the laryngeal complex, the hypothesis is that resistance training for hyolaryngeal excursion is possible.

Picture from Shaker, 2016, titled: Effects of laryngeal restriction on pharyngeal peristalsis and biomechanics: Clinical implications.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4935483/
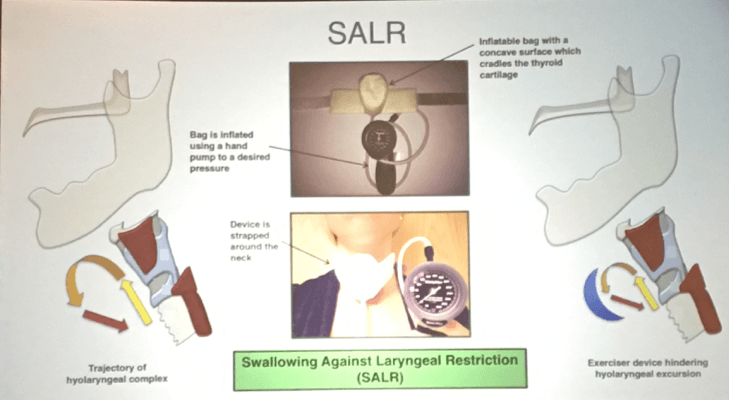
Slide from this session at DRS 2018, Baltimore, MD.
Dr. Agrawal and his team studied a group of 28 normal healthy participants, who were given either the device or a sham treatment for 6 weeks (exercising 3 times daily with increasing resistance over time). They were assessed via both Videofluoroscopic SwallowStudy.com (VFSS, aka, Modified Barium SwallowStudy.com/MBSS) as well as High Resolution Pharyngeal Manometry (HRPM). Results were favorable for the SALR treatment group versus the sham group with greater improvements noted in:
- UES opening,
- hyolaryngeal excursion, and
- posterior pharyngeal wall thickness (which was used as a surrogate for reductions in sarcopenia).
- The SALR group also had greater pharyngeal pressure on HRPM than the sham group.
15. High resolution pharyngeal manometry is being used clinically for better assessment of pharyngeal swallow.
From a sessions titled Pharyngeal High Resolution Manomtery and Videofluoroscopy presented by Dr. Tim McCullough and High Resolution Manometry with Impedance by Dr. Charles Cock
Speaking of what tools are in your dysphagia toolbox, since #15 is the end of our series, I could not leave you without mentioning High Resolution Pharyngeal Manometry. It was not a new topic for me at DRS this year, but it remains one that I do not yet have any clinical experience with, nor do the colleagues with whom I work day in and day out. Years ago, when I first learned of it, it felt like it was at an unattainable skill area for me — something that was being used in research only that was not directly clinically applicable for those of us “in the weeds” of clinical practice day in and day out.
However, at this year’s DRS meeting, I was pleased to see that is no longer true. HRPM is being used in clinical settings. Regularly. By “regular clinicians,” not just researchers. Its clinical utility is being proven more and more as the months and years go by. Drs. Timothy M. McCollough and Charles Cock, along with other colleagues on their panel, did a nice job providing an overview for all of us about the benefits of combining HRPM and VFSS/MBSS or HRPM with impedance (aka, manometry results with the pressures against the catheter from swallowing a bolus). Dr. Cock specifically pointed out that this method can:
- be performed by the SLP,
- assess the presence of the bolus and intrabolus pressures, and
- assess UES opening without direct visualization.
He explained how we can “see” things like spillage (aka, posterior escape of the bolus before the swallow trigger, but we still cannot tell if it is an oral delay with decreased bolus containment versus a true pharyngeal delay) or residue without a VFSS/MBSS or a FEES. He reviewed literature showing that there’s an 85% correlation of HRPM results with the Penetration Aspiration Scale. Dr. Cock made the case for using HRPM with impedance as a way to determine risk levels and further determine who would benefit most from the potentially less available objective tools like VFSS/MBSS and FEES.
DRS Dysphagia Digest Summary:
So, 15 fascinating points later, I’ll leave you with that question from above. What tools are in your toolbox?
“I suppose it is tempting, if the only tool you have is a hammer, to treat everything as if it were a nail.”
(This old saying has seen many revisions over the years, but this particular one is attributed to the psychologist Abraham Maslow in 1966, per quoteinvestigator.com)
I find attending DRS is a great venue to learn what more I can and should be doing for my patients beyond the “same old things.”
It is our responsibility as practicing clinicians to know the research well enough to advocate for what our patients need, based on the pathophysiology of the person’s swallow. In other words, first customize the evaluation process based on your hypotheses (making appropriate referrals as needed), and then customize the therapy plan, techniques and tools based on the specific structural, physiological, and/or behavioral issues you and the team find.
This post is part 3 of a 3-part series. Keep in mind; many of these studies are still in process. Where possible, we’ll point you to citations and primary literature to read. But in many cases, you’ll need to wait months (if not longer) for final results to be out on this data. This gives you all the more reason to regularly attend the Dysphagia Research Society’s Annual Meetings. The next one is in sunny San Diego from March 7-9, 2019!
In the meantime, we encourage you to read other work on related topics by these authors. Links provided to their research where possible. But never hesitate to trot on over to https://pubmed.ncbi.nlm.nih.gov and take a peek around for yourself! You can even use the “Open Access [filter]” in PubMed to find the free-open-access articles available. See also: https://www.ncbi.nlm.nih.gov/pmc/tools/openftlist/
Thank you again to my guest blogger:
 Amanda Warren, MS, CCC-SLP, is a medical Speech-Language Pathologist practicing in the city of Boston, MA. She has extensive experience in outpatient, acute care, rehabilitative care, skilled nursing and home care environments. Amanda teaches in Speech-Language Pathology at the undergraduate level at Gordon College and at the graduate level at Boston University. She is an author of continuing education courses at Northern Speech Services. She has a special interest in palliative dysphagia management, augmentative communication at the end of life, and patient-family advocacy and education.
Amanda Warren, MS, CCC-SLP, is a medical Speech-Language Pathologist practicing in the city of Boston, MA. She has extensive experience in outpatient, acute care, rehabilitative care, skilled nursing and home care environments. Amanda teaches in Speech-Language Pathology at the undergraduate level at Gordon College and at the graduate level at Boston University. She is an author of continuing education courses at Northern Speech Services. She has a special interest in palliative dysphagia management, augmentative communication at the end of life, and patient-family advocacy and education.