
Cotton Candy Therapy?
Transitional Foods as Potential Dysphagia Treatments
By Karen Sheffler, MS, CCC-SLP, BCS-S of SwallowStudy.com
 Got your attention with the cotton candy, didn’t I?
Got your attention with the cotton candy, didn’t I?
Imagine wandering through your town’s summer festival sucking that sickly-sweet cotton candy until it magically disappears on your tongue. What other foods start out as a solid and then change or transition into a liquid or a paste with the warmth and moisture of your mouth? (You know the dentists may not appreciate dysphagia therapists using cotton candy!) Common transitional food items that change in the mouth are ice chips, ice cream, some teething biscuits, and new therapeutic transitional food crackers (Barewal et al., 2021; Shune et al., 2022). However, not all teething biscuits or wafers safely dissolve in the mouth (more on that in Part 2).
Keep on reading to learn more about transitional foods, how to test them, and how to potentially incorporate these meltable snacks into dysphagia treatments.
Introduction to my 3-Part Article on Transitional Foods:
In Part 1 (below):
- Define Transitional Foods.
- Describe the oral condition and skills needed to process transitional foods.
- Describe how to test a Transitional Food, according to the International Dysphagia Diet Standardisation Initiative (see www.IDDSI.org).
- Provide ideas on their use in dysphagia treatment.
- Provide examples of transitional foods for people with dysphagia (e.g., the product EAT bar is no longer available, but Savorease™ products are available).
- Review the definition and statistics around choking.
- Discuss the dangers with some transitional foods (also known as first finger foods for 10-12 month olds to toddlers).
- Discuss the dangers with some transitional foods in this buyer-beware marketplace (e.g., some teething biscuits become rubbery and do not dissolve readily when they are NOT fresh out of the box).
- Warn against transitional food “imposters” that have been taken off the market due to choking (e.g., the Japanese snack of Konjac Jelly or Konjac Candy).
- Point out transitional foods that are extra challenging for people with difficulty swallowing/dysphagia (e.g., gelatin or Jell-O brand gelatin).
- Share how some transitional food items are used in dysphagia treatment in Japan and how these are different from the dangers of Konjac Jelly.
Disclosures: I will be primarily looking at this from my background as an adult & geriatric swallowing specialist, but as you will see below, most of the research is from the pediatric field. Additionally, I have nothing to financially disclose in mentioning any products within this article.
Definition & Analysis of Transitional Foods:
The International Dysphagia Diet Standardisation Initiative (www.IDDSI.org), placed the gray bar of transitional foods along the side of the diet framework pyramid, as they do not fall solely within one food or drink category.
How Does IDDSI Describe Transitional Foods?
Transitional Foods = start as one texture (e.g., a firm solid) and change to another texture when moisture is applied (e.g., saliva or water), or when a change in temperature occurs (e.g., heating).
Examples of transitional foods listed by IDDSI are:
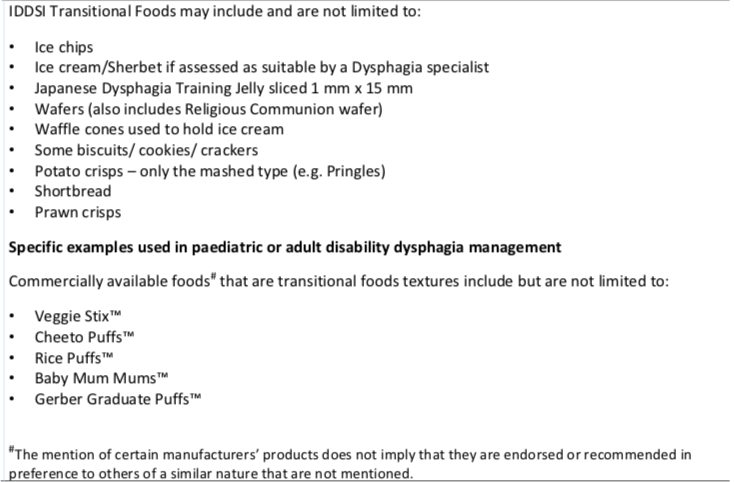
Transitional Foods. Caution: The term “crisps” is not a common word in the USA. That term is more common in the UK and Australia. They refer to a melt-in-your-mouth rice or potato crisp that is baked, not like the harder-fried potato chips in the USA. In the USA, only “Pringles” come close to a dissolvable potato chip, but I still would NOT consider than a perfect transitional food, as sharp particles remain even with applying tongue pressure. More on this in part 2.
Key aspects of a transitional foods:
- After the solid texture is altered by moisture and temperature, then
- Minimal chewing is required.
- Tongue pressure alone may be sufficient to break down these items.
Transitional Foods DO require:
- Direct supervision to ensure safety,
- Attention to task (not impulsivity or shoving the entire biscuit in the mouth at once),
- Heat and sufficient moisture in the mouth to start the break-down process,
- At least some up and down motions of tongue to palatal surface (aka, tongue pumping) to mash the item, and
- Some sucking and/or front to back tongue stripping across the palate to move a food from the front of the mouth to the back of the mouth. The ability to raise the tongue dorsum or tip to the palate will help strip residue off the palate. (These motions can be seen most definitively on fluoroscopy/motion x-ray.)
Transitional foods DO NOT require:
- biting (for adults, small 1.5 cm pieces can be placed in mouth; for children, 8 mm size pieces can be used),
- tongue lateralization to place the food on the back teeth for chewing, or
- grinding with a rotary chewing pattern at the molars.
We need to analyze each item to determine if they break down into a paste, a thick or viscous liquid, or to a thin liquid (such as with ice chips, popsicles, ice cream and gelatin/Jell-O). The person’s swallowing therapist would have to evaluate the person’s swallowing structure and function carefully to determine if the item is safe and if it is providing the desired therapy effect. Typically, when a food melts into a paste, we assume that it will be easier to swallow. However, that is not true for everyone. It depends on the type of difficulty swallowing (dysphagia).
For example, a person with oral dysphagia, but with an adequate pharyngeal swallow timing and function, may be able to handle ice chips and ice cream melting out to a thin liquid. (I often caution against Jell-O or any gelatin with people who have difficulty swallowing, as these require a whole lot of oral control as those slippery pieces break apart!) Our person with oral dysphagia may need the item to predictably dissolve to a thin liquid to prevent a loss of the item out of the oral cavity into the throat. Thorough dissolving will also help prevent oral residue.
If someone also has a pharyngeal dysphagia or a throat issue causing difficulty swallowing, then they may end up with food left behind along the back of the tongue and in the throat if the transitional food dissolves into a dry-sticky paste. Transitional food selection will have to be done carefully. They may also have to avoid a transitional food that melts to a thin liquid (e.g., ice cream and Jell-O), to avoid getting the thin liquid down the wrong way into the lungs (aspiration).
These issues are best analyzed by a speech-language pathologist or SLP (i.e., an SLP who specializes in swallowing and dysphagia). They may require an instrumental evaluation (e.g., Fiberoptic Endoscopic Evaluation of Swallowing/FEES or Videofluoroscopic Swallow Study/VFSS). These instrumental evaluations are the only way to see if the person is clearing viscous liquids and purees/pastes through the pharynx, as no specialist has bedside x-ray vision! Fortunately, researchers are currently investigating the safety of transitional foods with VFSS, and they are finding that there are no significant differences between transitional foods and purees when assessing oral and pharyngeal swallowing parameters on videofluoroscopic examinations (Shune et al., 2022). Using the VFSS or FEES, you will also be able to assess if the person is protecting the airway as the transitional food melts into a thin liquid and spills to the throat. These instrumental examinations can test a variety of transitional foods, thin liquids, and mixed consistencies.
Your swallowing specialist will make sure you have sufficient saliva to break down these transitional solids. Some people with dry mouth (xerostomia) may find some transitional foods to be sticky and NOT easy to swallow, requiring sauces and dips.
Testing Transitional Foods:
Play with your food! In order to analyze the safety of transitional foods for your patients and loved ones, you have to play with it, in other words – test it. In addition to this testing method below, you need to put it in your mouth and feel it. Can you hold it in your mouth with minimal tongue pumping and it just dissolves?
The following testing methods are per the IDDSI website and documents: Complete Framework document and Testing Methods.
Instructions for the Transitional Food Testing Method:
 1) Apply 1 ml of water to the sample. (Done here via syringe.)
1) Apply 1 ml of water to the sample. (Done here via syringe.)
Your sample could be a bite-sized piece of 1.5cm x 1.5cm.
Sorry, my sample in the picture is a larger.
2) Wait 1 minute.
3) Perform the IDDSI Fork Pressure Test (or chopstick test or finger test as described by IDDSI):
 a. Use a standard fork
a. Use a standard fork
b. Apply pressure to the base of the fork with your thumbnail until your thumbnail blanches white.
c. The sample should melt, disintegrate or squash. Leaves indentations from the fork. It does not return to its original shape when the pressure is released.
Now that you understand how the food feels in the mouth and throat, what oral processing skills may be needed, and how much moisture, heat and pressure is needed to break it down — you are ready to think about using different transitional food items in therapy.
Transitional Foods in Dysphagia Treatment:
One pillar of dysphagia treatment is diet modification; however, this cannot be done without the other pillars of compensatory strategies and rehabilitation/skill training. How do we train skills to upgrade a person’s diet without causing a choking episode on that “training” piece of chicken?!
Can transitional foods be used to more safely train these biting, chewing, lingual lateralization and bolus formation skills needed for more challenging foods? Can they also be used to advance a diet in cases of oral sensitivity and solid food refusals (often seen in the pediatric and geriatric populations)?
There is minimal research to guide us in using transitional foods in therapy. IDDSI recommended only two articles within their information on transitional foods (Gisel, 1991 and Dovey, Aldridge & Martin, 2013).
Therapy Goal 1: Getting someone off puree!
Imagine an acute stroke patient whose instrumental evaluation confirmed significant oral dysphagia, but with an adequate pharyngeal swallow and airway protection. The videofluoroscopic swallow study recommended puree and thin liquids. The person complains that she does not want to be on baby food. How will we train the oral preparatory skills required to return some quality of life in eating? When does she have adequate chewing durations and chewing cycles to manage solids more challenging than a puree?
We look to pediatric research to analyze the chewing durations and chewing cycles needed to process solids, gelatin (one time of transitional food) and purees. Gisel (1991) studied 143 healthy/typically developing children from 6 months old to 24 months old to analyze the effect of food texture on the development of chewing. Gisel defined:
- chewing duration as the time in seconds between placement of the food in the mouth to completion of the swallow (maybe a bit to broad).
- chewing cycle as one down-and-up movement of the mandible.
- Increased eating efficiency as a decrease in chewing duration.
The duration to cycle ratios were closely linked and similar for all three textures of a solid (Cheerios), gelatin (10 x 4 x 4 mm and 5 x 4 x 4 mm) and puree. Fewer chewing cycles were required as the children developed. For purposes of this discussion of transitional foods, it is important to note the findings that less time and fewer chewing cycles were needed for gelatin versus a solid. The children finished a bite of gelatin in 1/4thto 1/3rdthe amount of time needed for eating cheerios. Also, as expected, the bite of puree needed ½ to 2/3rdthe amount of time needed for the gelatin. The puree was even faster in comparison with a solid, consuming a puree in 1/7thto 1/4thof the time. Overall, Gisel commented that the difference between the gelatin and the solid texture was more significant. The significant limitations of this study are in the foods selected. The “solid” texture was a cheerio, which some may consider to be close to a transitional food, as it starts dissolving when held in the mouth. Then Gisel described “gelatin” a “viscous” texture, which it is not. Most gelatins (i.e., Jell-O) melt down to a thin liquid, requiring much less chewing effort and oral manipulation than a solid, which is why the greatest difference was found between the “solid” and the gelatin. Gelatin cannot be considered a food texture on a continuum between a puree and a solid. Clearly, more research is needed now that IDDSI has defined our diet framework and food categories for better research analysis.
To read more on how to quantitatively assess chewing and swallowing of solids, our homework will be to read Huckabee, et al., 2018, regarding the Test of Masticating and Swallowing Solids (TOMASS). See full reference below. See also my blog on testing mastication.
Therapy Goal 2: Desensitization to advance to more challenging food textures.
In addition to helping patients move up the food texture continuum, transitional foods may be beneficial for people who may have oral sensitivity issues, which may cause food refusals. Dovey, Aldridge & Martin (2013) noted that:
- oral sensitivity is “deriving insult from actual or imminent interaction with the mouth (i.e., touch) or through oral mechanicostimulation (i.e., chewing),” and is differentiated from taste aversions (Dovey, et al., 2013, p 502).
They studied a behavioral strategy for oral sensitivity. After initial stages of desensitization to allowing touch to the face and lips, they encouraged getting the face “messy” when playing with food. The second step was to read a story that included touch to the tongue and teeth. The third stage involved introducing a transitional food item. It involved a chewing protocol that eventually had the children chewing foods with their back molars. Researchers used an airy potato powder baked into a “crisp” (called Pom Bear). They defined these crisps as a transitional food as they “melt in the mouth after a period of time and can then be swallowed without the need to chew” (Dovey, et al., 2013, p 504). The introduction of these solids was to first interact with the crisps by breaking them into pieces. Desensitization progressed to placement of the crisps in four locations in the mouth (cheeks, between lips and teeth and under the tongue). The child had to retrieve it and spit it into a bowl using the tongue. The eventual chewing task analysis included:
- placement of the crisp on the back molars,
- biting,
- moving the jaw up and down in a chewing motion,
- opening the mouth to see if the crisp was swallow ready,
- continuing to chew, then
- using the tongue to swap the bolus to the other side of the mouth to
- continue chewing until ready to swallow,
- thus mastering the dominant and non-dominant sides.
This systematic task analysis of how to teach the management of a solid is good for us clinicians who work with the geriatric population as well. Age appropriate items could be used. This 3rd stage progression would train oral control, lingual control/bolus manipulation, chewing and tongue lateralization to move the bolus from one side to the other. The key is to use a transitional solid that will have a much lower risk of choking while these skills are being developed or rehabilitated.
*******
Transitional Foods – Product Examples:
(Disclosure again!: I am not receiving any financial incentive to mention these products.)
Products:
TheEATBar
This transitional food blog was inspired by me tasting, testing, and analyzing a product called TheEATBar. One of the founders, Tia Bagan, MS, CCC-SLP, sent me some products to sample. My family and I were hooked. My son ended up eating so many of them, that when I pulled out the chocolate package to have my 93 year-old mother-in-law try them, there was less than 1/2 of a biscuit left. My son and I are partial to chocolate anything, but the other flavors were delicious too.

This product used to be labeled as “EAT,” but is now called: “theEATBar.” Go to their website: https://www.theeatbar.com/ for info.
Bagan described theEATBar as a “product that is a high-calorie melt-away snack.” These yummy snacks have the potential for improving quality of life for people working to get off of pureed foods. They also may increase the acceptance of an easy to swallow solid for children through geriatrics with refusals, oral sensitivities, fear of swallowing, fear of choking, and food intake disorders (e.g., see the National Eating Disorder.org’s article on ARFID/Avoidant/Restrictive Food Intake Disorder). Note that ARFID can occur at any age – children through the elderly. ARFID is a newer term and is not the same as other common eating disorders (i.e., anorexia and bulimia), as there are no body image issues with ARFID.
Swallowing evaluations and treatments should always be done under the guidance of your medical team that includes your speech-language pathologist who specializes in dysphagia. That is a matter of life or death! (That said, more on hazards and choking risks in Part 2 of this blog).
Each box comes with three bars or biscuits providing 200 calories and 3 grams of protein. (Bagan noted that they package the bars individually as well.) Total carbohydrates are 30 grams with 29 grams of sugar. These are definitely a treat, and not for people with diabetes.
TheEATBar passed the IDDSI Fork Pressure Test when 1ml of water was added (see pictures and methods above). Here is another YouTube video of the Fork Pressure Test used on Transitional Foods.
When I tested a bite, I tried to just hold it in my mouth and use as little oral preparatory movements as possible. I did not chew at all. I found that I needed only a little tongue pumping or up and down movements. The bite started to change shape and consistency within 10-12 seconds. Then it dissolved into a smooth paste by 22-25 seconds. By 30 seconds, I just needed to use my tongue to clear trace residue off my palate. After a few swallows, the bite cleared within 35 seconds. (Note: I tested this several times with fresh biscuits and with biscuits that had sat opened for weeks. Timings will vary with the individual.) My first reaction was that it took some sucking and tongue pumping movements, but certainly easy to swallow, as you do not have to chew or lateralize the tongue. Because the biscuit is easy without chewing or using tongue lateralization, it could be used in therapy to safely train these skills.
My son was good at testing too (and for reference, he is 11 years old). He hardly moved his jaw or tongue while holding the bite in his mouth. He showed me how the bite was starting to melt and deform at 27 seconds. Then at 38 seconds he showed how there was some residue on his palate. And yes, he said the word “palate.” After a few swallows, he showed how it was gone at 45 seconds. He was observed to do 5 swallows total, with the first swallows of saliva during the holding period. Right before he took another bite, he said: “It’s gone. Totally gone. Yeah, this is good!”
Savorease™ Therapeutic Foods
Savorease is for adults and children. Savorease is a similar transitional food product, and research has shown that it has excellent dissolvability and safety, even for people with dry mouth and/or dysphagia (Barewal et al., 2021; Shune et al., 2022). I talked with the owner (Dr. Reva Barewal , Founder, Oral Reconstruction Specialist, and Culinary Chef) several times in her early days of creating this company. I have been a long supporter and tester of the company’s products and mission. Love the samples at many conferences! What is truly important about these products is that it returns a sense of savory food texture, as these transitional food items have been found to leave less residue than a pureed food. See research shared on the Savorease website and presented at a Dysphagia Research Society meeting.
*******
Thank you for reading and sharing.
Please use the comment section below to add thoughts or questions. I would love to hear from my pediatric colleagues, as transitional foods have been used more often in the pediatric population.
For more information on IDDSI, follow the links above to the IDDSI website and framework. Go to the Resources section on the IDDSI website often, as they are frequently adding to that section to assist therapists in implementing this standardized diet. Download your free IDDSI App on your phone or device today. Check out my IDDSI links and blogs on this page linked here.
Check out Part 2 & Part 3.
Transitional Foods References:
Gisel, E.G. (1991). Effect of Food Texture on the Development of Chewing of Children Between Six Months and Two Years of Age. Developmental Medicine & Child Neurology, 33, 69-79. doi:10.1111/j.1469-8749.1991.tb14786.x
Dovey, T.M., Aldridge, V.K. & Martin, C.I. (2013). Measuring oral sensitivity in clinical practice: A quick and reliable behaviouralmethod. Dysphagia, 28(4), 501-510. https://doi.org/10.1007/s00455-013-9460-2
Huckabee, M. , McIntosh, T. , Fuller, L. , Curry, M. , Thomas, P. , Walshe, M. , McCague, E. , Battel, I. , Nogueira, D. , Frank, U. , den Engel‐Hoek, L. and Sella‐Weiss, O. (2018). The Test of Masticating and Swallowing Solids (TOMASS): Reliability, validity and international normative data. International Journal of Language & Communication Disorders, 53, 144-156. doi:10.1111/1460-6984.12332
New references as of 2021-2022:
Bayne, D., Barewal, R. & Shune, S. (2022). Sensory-enhanced, fortified snacks for improved nutritional intake among nursing home residents. Journal of Nutrition in Gerontology and Geriatrics, DOI: 10.1080/21551197.2022.2025971. https://doi.org/10.1080/21551197.2022.2025971
Barewal, R., Shune, S., Ball, J. et al. (2021). A Comparison of Behavior of Transitional-State Foods Under Varying Oral Conditions. Dysphagia, 36, 316-324. https://link.springer.com/article/10.1007/s00455-020-10135-w
Shune, S., Bruno, E. & Barewal, R. (2022, March). In vivo behavior of transitional foods as compared to purees: A video fluoroscopic analysis. Poster presented at: Dysphagia Research Society Annual Meeting, Kimberly Wisconsin. See poster here (shared by Dr. Barewal).