
Think Outside the (Pill) Box:
3D Printed Pharmaceuticals
Meeting the Unmet Need of People with Difficulty Swallowing Pills (Pill Dysphagia)
By Karen Sheffler, MS, CCC-SLP, BCS-S of SwallowStudy.com
Introduction to Pill Dysphagia
You may hear this often in healthcare: “He is non-compliant with his medications.” “She is really bad at taking her pills.”
Have you heard a doctor say that before? Have they considered how difficult it is to swallow pills? (Not to mention the costs and the extreme complexity of taking many medications in the right amount, at the right time, and in the right way.)
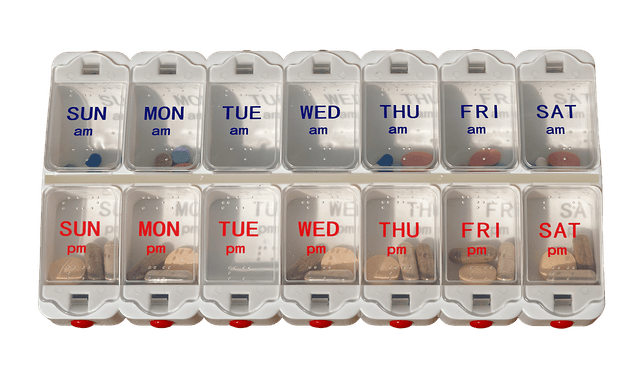
This is a 2-tiered pill box, showing morning and nighttime pills. Some pill boxes are even more complex with 4-tiers, showing morning, noon, dinner and night. It is a complex cognitive task to fill a pill box. The person has to be oriented to the day and time of day to take the correct pills.
Imagine the grandfather with advanced Dementia, who has difficulty swallowing pills and cannot understand the medical need for those 20 drugs that fill his pill box. His granddaughter tries to make the task safer and easier by crushing all his morning pills and placing the mixture into applesauce. One taste of that nasty-bitter concoction has him spitting out all those expensive and necessary medications. Will his doctor see his high blood pressure as medication non-compliance?
Even for people who do not have difficulty swallowing, taking a large pill with a sip of liquid is a challenging task, especially for children. Just the other day, when I tossed a slippery Vitamin D into my mouth, it rolled back into my throat before I was ready to swallow it! That lead to a lot of coughing!
Read my other blogs about Pill Dysphagia and what you can do about it here.
Then, step into the future with me and read on, as I show you how 3D printing will transform the pharmaceutical industry.
The Revolution of 3D Printed Pharmaceuticals
“3D printing is another approach to advanced manufacturing. These methods are capable of manufacturing pre-determined 3D geometric structures of solid drug products in various shapes, strengths and distributions of active and inactive ingredients. This approach provides a unique opportunity to produce medicines that are tailored for individual needs of patients,” per Scott Gottlieb, the FDA Commissioner, in a blog on July 13, 2018. Here is a 2017 article by same author, as that 2018 link is now broken.
“I anticipate a slow but really profound revolution in what we think of as a finished drug product over the next 10 or 15 years,” said Janet Woodcock, MD, Director of the Center for Drug Evaluation and Review at the Food and Drug Administration (FDA).
Dr Woodcock, MD spoke at a conference on 3D Printed Pharmaceuticals in Livingston, NJ on November 8, 2018. This first ever Summit on 3D Printed Pharmaceuticals was sponsored by the Center for Medicine in the Public Interest (CMPI.org) and Aprecia – The 3DP Pharmaceutical Company.
I was invited to speak at this conference to increase awareness about people who have difficulty swallowing (dysphagia). I shared the struggle that people go through every day to swallow foods, liquids and pills safely (i.e., keeping things out of the airway) and efficiently (i.e., not leaving items stuck in the mouth, throat or food tube to the stomach/esophagus). I reminded the audience that dysphagia is not a disease itself, as there are many different diseases, disorders, and structural and functional abnormalities that can lead to difficulty feeding, eating and swallowing. This perspective helped the scientists, researchers and industry partners begin to understand why they are working so hard to make pills easier to swallow. The inspirational conference was about fostering innovation without losing sight of the individual.
“What is meeting that patient’s need? I said that as patient’s (with an apostrophe-s) need or needs, because we’ve done patients’ needs… the one-thing-fitting-all approach,” emphasized Tim Tracy, Chief Executive Officer of Aprecia® Pharmaceuticals.
Dr Robert Goldberg, Vice President of the CMPI, stressed that it is time for action, as “it would be a tragedy” if we do not address the unmet need of people dealing with swallowing disorders. I have written before on “hope” in dysphagia management, but this is real-tangible hope happening in research and industry now!
Dr Woodcock noted that the FDA has approved the 1st 3D printed dosage form, which is called ZipDose® technology and was created by Aprecia®. She is very aware of the challenges that people deal with when they have so many pills to take, along with the difficulty in swallowing them. She agreed that crushing pills and putting them in applesauce is “not satisfactory.”
“These patients are sicker and really need the medications, but they are less likely to take them as it is so burdensome,” said Dr Woodcock.
She is encouraged by technological advances in 3D printed pharmaceuticals, which can print or spray medication into many customizable dosage forms. She dreams of a day when we can have “pharmacy-on-demand.” Imagine your specific targeted medications sprayed out by a 3D printer in your own pharmacy. Maybe one porous wafer or tablet will contain your multiple drugs. It will easily melt in your mouth with a pleasant taste and be easy to swallow.
The future is bright!
Reducing Pill Burden & Addressing Unmet Needs
Let’s take a closer look at this burden due to difficulty eating and swallowing.
As noted above, people can have difficulty swallowing (dysphagia) with foods, liquids and pills. Even saliva can be hard to swallow for some people. Others may have the issue of gastroesophageal reflux (i.e., where the lower esophageal sphincter, which should close back up after the swallow, ends up inappropriately relaxing and allowing stomach contents to come back up the esophagus). Some people may have food, liquid and pills remaining in the esophagus, never reaching the stomach; this can cause a risk for the items to come back up after eating and get into the airway. Still more people suffer from gastroparesis, which affects the stomach contractions and stops or delays stomach emptying, leading to feeling full quickly, nausea, bloating, refluxing and vomiting.
Pills can get stuck all over the place! Pills can become pocketed in the mouth and cheeks with people who have had a stroke and one side of the mouth is weak. Others may have difficulty just getting the pill out of the mouth due to fear of swallowing the pill or increased confusion. Pills can get stuck in the throat due to a slow, weak and/or discoordinated swallowing, leaving pills sitting in the multiple pockets in the throat and not stripped through to the esophagus. When pills remain in the esophagus for too long, it can cause pill injury (an erosive damage to the lining of the esophagus).
One of the most challenging swallowing tasks is to wash pills down with a drink of water. If you do not swallow in a timely fashion, with quickly and tightly closing up your airway/voice box (also called the laryngeal vestibule), then the liquid can get down the wrong way into the lungs. Even the pill itself can fall into the airway. Material falling into the airway and dropping into trachea that leads to the lungs is called aspiration. Aspiration over time, in conjunction with a reduced immune response and poor oral hygiene, can quickly turn into an aspiration pneumonia (especially in our bedridden grandfather with advanced Dementia).
With all that can go wrong, we need to look to scientists, researchers and industry to help people reduce their pill burden.
NOTE: To thoroughly figure out at what level of difficulty you are having with swallowing, we have to do instrumental dysphagia evaluations to figure out why you are having trouble and what we can do about it. (See also this blog on how do I know I need a swallowing or dysphagia evaluation.) Here is a good example of an elderly woman having a lot of trouble swallowing a pill (the videofluoroscopic swallow study is one example of an instrumental dysphagia evaluation). See the full YouTube description at the end of this blog if you want more details on what you are seeing.
The Wonders of a 3D Printed Pill
Now that you realize why we have to care and take action: Check out these quick videos to really see how amazing this 3D printed pharmaceutical technology platform is.
NOTE: The video suggests that you need a sip of liquid for the tablet to dissolve; however, I found that the ZipDose® tablet dissolved quickly in the mouth with just my saliva (similar to a “transitional food” item – see blog for more information. The key factor there is the potential need for normal salivary quantity and quality – see this saliva blog). Some people with dysphagia may not be able to take a sip of thin liquid (water), as taking a sip of liquid may cause the particles to wash into the lungs with an aspiration. If the person is drinking thickened liquids, you do not want to add the polymer of a thickened liquid to the medication particles, as that could bind with the medication and make it less bioavailable to the body (See this blog on swallowing medications).
The Benefits of 3D Printed Pharmaceuticals
- The porous, orally disintegrating tablet can dissolve quickly in the mouth. The video above shows how Aprecia is “redefining fast-melt technology,” as noted on their website Aprecia.com.
- Meets many unmet needs beyond those of dysphagia, such as for people with gastroparesis who may need pre-gastric absorption. Michael S. Smith spoke at the conference on behalf of Gastroparesis Patient Association for Cures and Treatments (G-PACT.org), which he co-founded.
- Has a long shelf-life, which is good for emergency preparedness, for countries or locations without potable water, and for personnel on the battlefield.
- Customizable geometry, hardness, and composition.
- Imagine fun shapes for kids.
- You can tailor the dosage to the individual in the 3D printing process. It is highly accurate at very low doses (e.g., 1 microgram) or very high dosage amounts, both of which are hard to do in traditional pills. For example, in traditional manufacturing, when the load of active pharmaceutical ingredients (APIs) goes up, the tablets have to get bigger and harder to swallow, per Dr Jae Yoo, Chief Technology Officer and co-founder of Aprecia Pharmaceuticals. “Traditional pharma techniques were limited to low dose compounds,” stated Dr Yoo.
- You can adjust the release rates or create a complex release profile to meet an individual’s needs.
- Anti-counterfeit features can be added, per Dr Jae Yoo. There can be patient-level authentication, as the patient can break the tablet and see a code inside. Counterfeit tablets in the market could cause serious consequences or death.
- Tablets are created layer by layer without compression force that may break particles. There are no molds. You control all the layers; for example, there may be a hard shell and an inner core that falls apart easily or can have liquid chambers. Dr Jae Yoo noted how more potent drug compounds can be put into the center of the tablet so people are protected from some potentially toxic compounds.
- Ease of modifying the dosage in a specific tablet. (In traditional pharma production, you may have to disrupt the production rate considerably to run a new batch with a different dosage amount. This causes “a lot of delays in the manufacturing cycle,” per Dr Yoo.)
- Combination therapy: Multiple medications could be inserted into chambers of one orally disintegrating tablet, further reducing the pill burden of taking multiple medications (polypharmacy).
- More palatable than crushed medications.
- Accelerated development cycle: Makes drug development more efficient, going from research to market faster for more patient benefit. Adam Procopio, Senior Principal Scientist at Merck, thinks that this can speed up the phase 1 through phase 3 drug trials, shrinking the cycle time to get medications to the people faster.
- Distributive manufacturing and marketing: imagine your pharmacy printing onsite and on-demand based on your personal clinical parameters, your current dosage adjustments, and your specific release rate profile.
Innovations Will Get Us Out of a Rut
Dr Woodcock sees that the drug manufacturing industry has been “stuck in a rut for over 50 years,” but she noted that the FDA takes some responsibility for where we are today. One issue has been prioritizing regulations over innovation. Other issues like outsourcing and off-shoring have broken up the manufacturing process into many different countries, causing long supply chains. Long supply chains can lead to drug shortages. I was shocked by the length of some supply chains. For example, per Woodcock’s description, active pharmaceutical ingredients (APIs) may be made in the United States, then the secondary processing may happen in another country, the finishing into the final dosage forms is done in a 3rd location, and finally the labeling and packaging may be done in yet another country! This is risky business. A natural disaster or other emergency could completely disrupt these long supply chains that we usually take for granted. We may not be able to reach that stock pile of medications in an emergency situation. Dr Woodcock spoke of regionalization, redundancy and smaller manufacturing units, especially for the future of smaller targeted populations who are receiving personalized or precision medicines.
Personalized Medicine & 3D Printed Pharmaceuticals
The concept of 3D Printed Pharmaceuticals is the perfect companion to the current state-of-the-art in medicine, which is a personalized medicine approach (aka, precision medicine or stratified medicine). This is targeting evaluations and therapies to the individual. Precision medicine is especially advancing in the field of cancer treatment. (See more definitions and references below). For years there have been the big “blockbuster” medications that have used a one-size-fits-all-approach. Maybe a given drug was really appropriate for about 4 out of the 10 people taking it. You may have 10 different reactions in those 10 people taking that same drug.
Dr Richard Smith (2012) argued in his article called Stratified, Personalised, or Precision Medicine that maybe patient “compliance” is low because “current medicine is imprecise.” “Because diagnosis is so imprecise, it follows that treatment will be haphazard.” Smith advocated for classifying people better by their individual response to medications and treatments. Maybe that in turn would lead to new ways of testing and classifying disease.
There is a shift in drug development under the precision medicine model, per Dr Woodcock, moving industry away from the blockbuster medication model to the specialty pharma model.
There will be the “need for manufacturing in a smaller scale, but at a higher level of technology,” stated Dr Woodcock.
Personalized medicine seeks to provide the right drug, at the right dose, for the right patient, at the right time. See this terrific infographic by the University of Illinois at Chicago:
https://healthinformatics.uic.edu/resources/infographics/how-tech-companies-are-changing-our-healthcare-system/
Summary 3D Printed Pharmaceuticals
The sense of urgency cannot be over-stated. Good thing this revolution has already started! As we all know, the Baby Boomers are coming: By 2030, >20% of our population will be over 65 (versus only 9.8% of the population was over 65 back in 1970).
Dr Goldberg, from CMPI.org, started the summit with the example of how suitcases with rolling wheels were initially invented in 1945, but that innovation did not take off until the 1990’s! Who can imagine a suitcase without wheels now? In 1945 there was no need for the masses to roll their suitcases quickly through an airport, so the technology was really slow to catch on. However, with 3D printed pharmaceuticals, the need is here now for the public. We have to continue to raise the awareness of people of all ages who have difficulty swallowing. Additionally, we cannot forget that this technology will be perfect to address the needs of children who cannot swallow whole pills yet and for all those people who are able but have fear of swallowing pills. With the need loud-and-clear, science and technology are ready to push the industry to new limits. The sky is the limit. “The nice thing about 3D printed pharmaceuticals is that it is something that the public and congress can understand… They get the concept,” Dr Janet Woodcock, MD, Director of the Center for Drug Evaluation and Review from the FDA, stated. We will only be limited by our imaginations.

Polypharmacy (taking more than 5 medications) is a challenge for many people. Remembering to take pills, swallowing pills, and adhering to complex plans are all challenges many adults face daily. Imagine how 3D printed pharmaceuticals could help — especially if we could dissolve one wafer in the mouth that has all our medications in it 3D printed for us by the pharmacy!!
I want to deeply thank all those involved with this first Summit on 3D Printed Pharmaceuticals for including those of us discussing the patient’s perspective and the medical perspective of dysphagia. This will be an exciting and innovative journey together.
Thank you for reading and looking into the future with me, as this future is NOW.
*******
Financial disclosure: I am not receiving any financial incentive for writing this blog or for including the organizations and company stated within this blog. I received reimbursement for travel and lodging expenses to speak at the 3DP Summit and my conference fee was waived, but I did not receive any additional financial honorarium.
*******
More Learning
Personalized Medicine Definitions:
(per Brice, P. (2015); Pokorska-Bocci, A. (2016, October) with phgfoundation.org/file/13380)
1. Stratified Medicine:
Grouping patients by clinical biomarkers, matching diagnostics and therapies (e.g., genetics can predict a given subgroup’s response to a particular drug).
2. Precision Medicine:
To tailor diagnosis and treatment to the individual. The term was used by the US Institute of Medicine. It is most advanced in oncology. Examples:
- Use of genomic information of a tumor or
- Use of molecular taxonomy of a disease.
- Delivering the optimal dose of the right drug to a specific patient with a very specific condition.
- Considering the individual’s genotype (set of genes in our DNA) and his/her phenotype (observable physical characteristics and the body’s biochemical makeup with all its environmental influences. How the genetic makeup is expressed).
3. Personalized Medicine:
An all-encompassing term for delivering medical care tailored to the individual, using new tools for diagnosis and treatment.
This combines new genomic medicine, biomedical discoveries, and big data (thanks to advances in medical information technology to collect and analyze our medical data). Personalized medicine also includes:
- Patient empowerment
- Patient-centered / Patient-directed medicine
- Lifestyle and environmental influences
- Preventative medicine
- Evidence-based therapy, based on patient’s specific profile. Speech-language pathologists who specialize in dysphagia strive to tailor a patient’s therapy to the specific pathophysiology behind why they are having aspiration and too much residue. We also are moving away from a one-size-fits-all approach. We need to tailor our evaluations to answer our clinical hypotheses, which are gathered from initial bedside/clinical evaluations. A thorough and more precise dysphagia evaluation process can lead to more targeted therapies and improved outcomes. I spoke at the American Speech-Language and Hearing Association’s annual convention in Boston in November, 2018 about how the field of dysphagia also needs a new “Platinum-Standard of Personalized Medicine.”
*******
References
Brice, P. (2015, February 2). Obama’s precision medicine initiative: The future of healthcare? Retrieved
September 5, 2018, from https://www.phgfoundation.org/blog/obamas-precision-medicine-initiative-the-future-of-healthcare
PHGFoundation’s latest report (England): Raza, S., Blackburn, L., Moorthie, S., Cook, S., Johnson, E., Gaynor, L. & Kroese, M. (2018, September). The personalised medicine technology landscape. Retrieved September 25, 2018, from https://www.phgfoundation.org/documents/phgf-personalised-medicine-technology-landscape-report-50918.pdf
Smith, R. (2012, Oct 15). Stratified, personalised, or precision medicine. Retrieved from
https://blogs.bmj.com/bmj/2012/10/15/richard-smith-stratified-personalised-or-precision-medicine/
Personalized Medicine Infographic:
Created by the University of Illinois at Chicago
https://healthinformatics.uic.edu/resources/infographics/how-tech-companies-are-changing-our-healthcare-system/
Recommended Reading on 3D Printing (John Hornick at the Summit on “Partnering for New Technologies in Medical Advancement”). This book and many video interviews can be found online by searching: “John Hornick & “3D Printing Will Rock the World.”
Hornick, John. (2015). 3D Printing Will Rock the World. Create Space Independent Publishing Platform. North Charleston, South Carolina.
*******
YouTube Description on Video: Pill Dysphagia Seen on a Videofluoroscopic
(SwallowStudy.com YouTube Channel)
Note: this description is for the public, as it does not go into the detail of WHY these issues are happening and what we did about it. The speech-language pathologist would further analyze the underlying problems to tailor strategies and therapy (i.e., structural deficits, timing or coordination issues, and speculate on the strength or motility of the entire swallowing process). It is very complex!
“Taking pills with liquids can be very challenging and dangerous! You can see this elderly woman sitting in the side-view position during a videofluoroscopic swallow study (aka, modified barium swallow study).
The pill is that black disc on her tongue as the video starts. When she washes the pill out of the mouth with liquid, she does have penetration of the liquid above the level of the vocal cords (in the voice box). She first has difficulty with the pill falling into her laryngeal vestibule (or voice box), just above the level of the vocal cords. The pill does not fall further into the trachea, but the risk is high. She then coughs 2 times, and the pill is stuck momentarily in a pocket at the bottom of the throat (called the pyriform sinus). You can see her pointing to it. More liquid penetrates as it washes the pill through the top of the esophagus. Then with all that liquid she took to get the pill down, the liquid starts coming back up on her (retrograde flow of liquid in the esophagus, with supraesophageal reflux, aka backflow of liquid out of the esophagus to the bottom of the throat). This is also dangerous for aspiration of the liquid after the swallow.
When the esophagus was scanned in the lateral position, you first see more of this retrograde flow of the liquid. Then you see the pill retention in the bottom of the esophagus (distal esophagus). She still felt it stuck in her throat, even though it was all the way down in the bottom of the esophagus. This is called a referred sensation, as the esophagus is not so smart at telling you where a ball of food (aka, bolus) or pill is stuck. People often feel like they are “choking” on a piece of food or a pill when it is actually stuck in the esophagus. That is the power of really seeing where things are with instrumental evaluations.
This video shows the reality of how hard it can be to swallow pills when you have difficulty swallowing (dysphagia).”
thank you.
That “admin” is just me alone (she/her pronouns – not “his”).
I am a speech-language pathologist who specializes in swallowing/swallowing disorders, and I am very dedicated and committed to patient safety and quality-evidence-based care!
thanks!